A New Spin on TAVR
Thanks to a Newly Approved Device, Aortic Regurgitation Can Now Be Treated Without Surgery
Transcatheter aortic valve replacement (TAVR) has revolutionized cardiac care, helping thousands of people with aortic stenosis (AS) avoid surgery while getting the care they need. Now, an innovative new valve is expanding TAVR’s reach to help patients with symptomatic, severe aortic regurgitation (AR).

The interventional cardiology team at Columbia University Irving Medical Center (CUIMC)/NewYork-Presbyterian Hospital (NYP) performed one of the first commercial implants of the Trilogy™ Transcatheter Heart Valve System — the first and only transcatheter device approved for symptomatic, severe aortic regurgitation (AR) in the United States.
Developed and manufactured by JenaValve Technology, Inc., the Trilogy System offers a safe and effective treatment option for patients living with AR who are at high risk for surgery.
“We're very excited to finally have a new, less invasive therapy for high-risk patients with aortic regurgitation,’ says Torsten Vahl, MD, Director of Translational Research and national principal investigator for the ALIGN-AR trial. “This device allows these patients to get treated without open-heart surgery.”

The Columbia/NewYork-Presbyterian structural heart team after performing one of the first commercial U.S. cases using the JenaValve Trilogy Transcatheter Heart Valve System for high-risk patients with severe aortic regurgitation.
The Challenge
Since 2011, transcatheter aortic valve replacement (TAVR) has been used to treat aortic stenosis (AS), a stiffening of the aortic valve caused by calcium buildup. Traditional TAVR uses those calcium deposits as a surface to anchor the new valve. Because TAVR is implanted using a catheter and guidewires, it is an attractive alternative to open heart surgery.
But with pure aortic regurgitation, the leaflets are typically not calcified. They remain thin and mobile, but because they don't close properly, blood flows back from the aorta into the ventricle.
In the absence of calcium, traditional TAVR valves have a tendency to migrate after deployment. Even if the device stays in place, TAVR used for AR has a higher rate of paravalvular leaks, meaning leaks around the new valve. “Overall, the outcomes were much worse when these devices were used off-label in AR patients than what we were used to from AS patients,” notes Dr. Vahl.
Which leaves the question: how do you keep a TAVR valve in place when there is no calcium?
The Solution
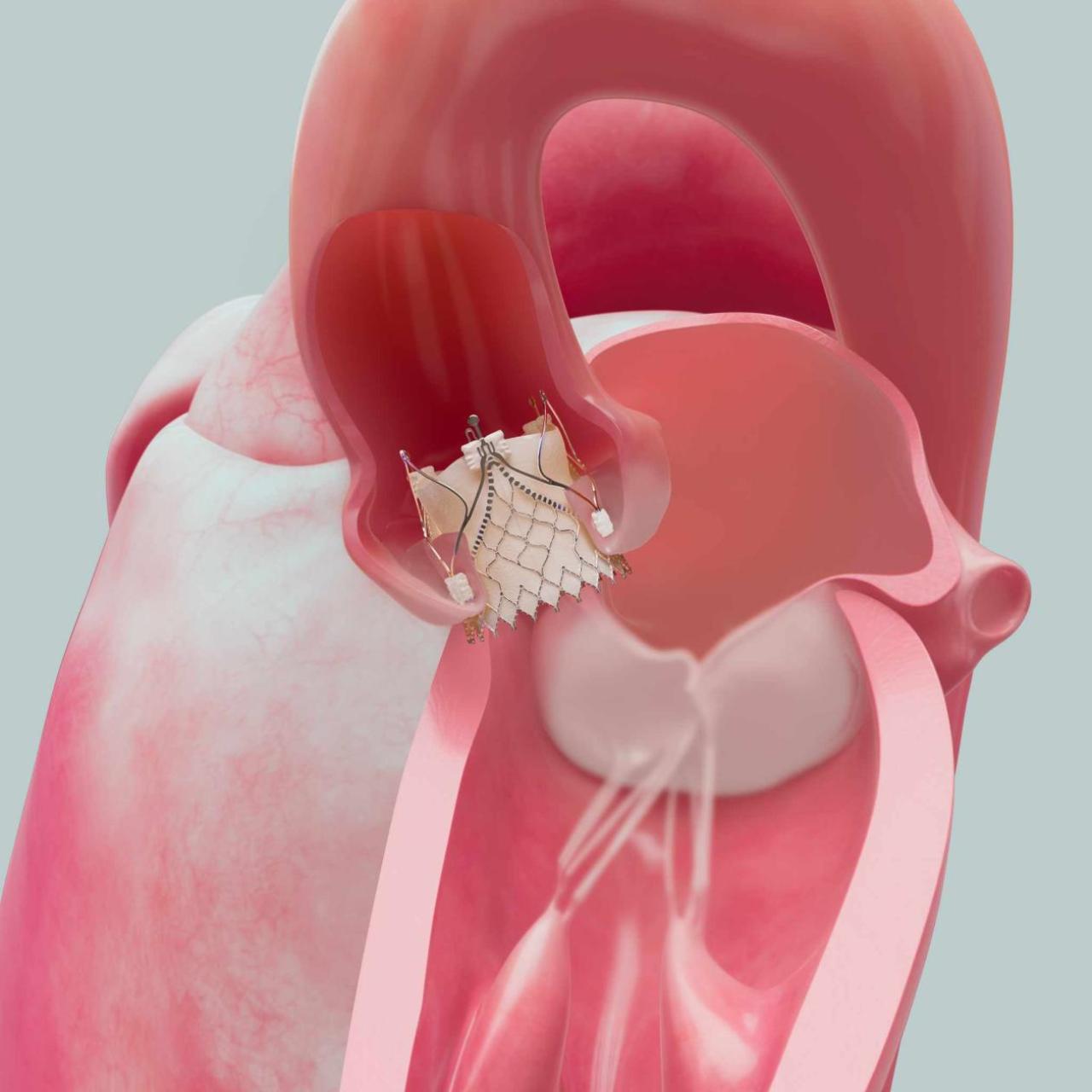
To address this, the Trilogy system uses three metallic anchors, or locators. Each of them is placed into one of the three cusps of the aortic valve, and the native leaflet then gets trapped between that locator and the actual body of the device.
‘It clips on like three paperclips,” says Dr. Vahl. “As a result, it can't migrate into the ventricle because the locator provides a stopping point when it hits the bottom of the leaflet. And the risk of it moving into the aorta is also lower.”
The native leaflets become an outer seal, creating a skirt around the valve. “This is why we think the paravalvular leak rates are low; even moderate paravalvular leak was found in only half a percent of patients in the ALIGN-AR trial.”
The stability of the Trilogy system offers several benefits. “Once you have this device in place, it can serve as an anchoring platform for additional TAVR valves to be placed inside of it in the future,” says Dr. Vahl. “And this technology can also be used for other high-risk groups, such as patients with left ventricular assist devices (LVAD). These patients sometimes develop aortic regurgitation, and by definition, they are considered high risk for open heart surgery, as they already have an LVAD.”
An Unmet Clinical Need
Currently, the standard treatment for severe AR is surgical aortic valve replacement using open-heart surgery. In fact, the American College of Cardiology (ACC)/American Heart Association (AHA) guidelines advise strongly against TAVR for patients with aortic regurgitation because of historically poor outcomes.
TAVR has only been performed as an off-label procedure in extreme-risk patients who had no other option. Commercial approval of the Trilogy system offers a much-needed option for some high-risk patients. “The ALIGN-AR trial only enrolled patients who were high risk for surgery, so at the current time, it should only be used in that population,” says Dr. Vahl. “But there are a number of high surgical risk AR patients that require aortic valve replacement that would otherwise not have been offered a treatment.’
AR patients with low and intermediate surgical risk should still consider surgical aortic valve replacement, but they can also explore new clinical trials. “They could possibly enroll in the ARTIST trial, where low- and intermediate-risk patients with significant aortic regurgitation are randomized to either open heart surgery or TAVR with the Trilogy device.”
Expanding Our Options
TAVR has become a genuine game-changer for treating AS. The Trilogy system now opens the door for patients with AR to gain the same benefits. “The older the patient gets and the higher their surgical risk, the more we try to find less invasive methods to help them with their problem. The intention is to avoid surgery in this setting because the patients recover much faster and require less rehabilitation.”
Dr. Vahl hopes that the new device will reduce the undertreatment of patients with aortic regurgitation. “When we started, no patients with aortic regurgitation were sent to our valve clinic. Cardiologists and primary doctors tried their best to medically treat their heart failure symptoms because there was no alternative therapy available for high-risk patients.”
“But now, we are adding an additional tool. I think this is very exciting news for our patients. If they have aortic regurgitation and heart failure symptoms, they should come and see us to be evaluated.”
Related